

Immigrant Health-Care Workers in the United States

Health-care workers supporting the U.S. COVID-19 response. (Photo: Jake Greenberg/U.S. Pacific Fleet)
Immigrants represent disproportionately high shares of U.S. workers in many essential occupations, including in health care—a fact underscored during the coronavirus pandemic as the foreign born have played a significant role in frontline pandemic-response sectors. In 2018, more than 2.6 million immigrants, including 314,000 refugees, were employed as health-care workers, with 1.5 million of them working as doctors, registered nurses, and pharmacists. Immigrants are overrepresented among certain health-care occupations. Even as immigrants represent 17 percent of the overall U.S. civilian workforce, they are 28 percent of physicians and 24 percent of dentists, for example, as well as 38 percent of home health aides.
Overall, immigrants ranging from naturalized citizens, legal permanent residents, and temporary workers to recipients of Temporary Protected Status (TPS) and the Deferred Action for Childhood Arrivals (DACA) program accounted for nearly 18 percent of the 14.7 million people in the United States working in a health-care occupation in 2018. As a group, immigrant health-care workers are more likely than their U.S.-born counterparts to have obtained a university-level education. Immigrant women in the industry were more likely than natives to work in direct health-care support, the occupations known for low wages. In contrast, immigrant men were more likely than the U.S. born to be physicians and surgeons, occupations that are well compensated. Compared to all foreign-born workers, those employed in the health-care field were more likely to speak English fluently and had higher rates of naturalization and health insurance coverage.
As the Migration Policy Institute (MPI) has documented, significant numbers of immigrant college graduates with health-related degrees are facing skill underutilization, in other words are working in low-skilled jobs (for example registered nurses working as health aides) or are out of work. This skill underutilization, often referred to as brain waste, affects 263,000 immigrants in the United States with college degrees—a workforce whose talents could be tapped amid the pandemic.
Even before the COVID-19 pandemic, a number of health-care occupations were among the fastest-growing occupations, as projected by the U.S. Bureau of Labor Statistics (BLS) for the 2018-28 period. The more immediate trends now are less clear. Like other parts of the U.S. economy, the health-care sector has suffered job losses since February 2020, which may continue until the economy rebalances. Nonetheless, the main drivers for a greater demand for health-care services—population aging and longevity—remain valid. As in the past, immigrants can be expected to play a significant role in the future of U.S. health care.
This Spotlight provides a demographic and socioeconomic profile of foreign-born health-care workers residing in the United States. The data come primarily from the U.S. Census Bureau's 2018 American Community Survey (ACS) and BLS. All data refer to civilian, employed workers ages 16 and older, unless otherwise noted.
- Historical Trends and Projections
- Number and Share Nationally and by State
- Region and Country of Birth
- Education, Naturalization, and Language Proficiency
- Visa Pathways
- Health Insurance Coverage
Pre-COVID 19 Trends and Projections
Health-care occupations employed approximately 14.7 million native-born and immigrant workers in 2018, up from 12 million in 2010. Before recent significant shifts in the labor market as a result of the COVID-19 disruptions to daily life, health-care occupations were projected to account for 1.9 million of the 8.4 million jobs expected to be newly created in the United States between 2018 and 2028.
Jobs in the health-care occupations fall into two broad categories: health-care practitioners and technical occupations (9.6 million workers in 2018), and health-care support occupations (5.1 million). Health-care support occupations were expected to grow the fastest among the 22 broad workforce-wide occupational groups analyzed by the U.S. Bureau of Labor Statistics (BLS), which pre-COVID-19 had been projected to increase by 18 percent between 2018 and 2028, followed by health-care practitioners and technical occupations (12 percent).
Several factors explain these upward projections. The aging and longer life expectancy of the U.S. population continue driving the demand for care and treatment of chronic illnesses. So do the aging and retirement of current health-care workers and those who teach in medical and nursing schools. The lengthy time needed to acquire education and on-the-job training in health-care occupations makes it harder, if not impossible, to switch between professions in response to new job opportunities, while professional licenses often restrict geographic mobility.
- Click here for more information about the BLS employment projections methodology.
Number and Share Nationally and by State
Among the 14.7 million workers employed in health-care occupations in 2018, 2.6 million (18 percent) were foreign born. The immigrant share of health-care workers was a fraction higher than that of all employed civilian workers ages 16 and over (see Table 1).
Relative to their share of the total workforce, immigrants make up disproportionate shares among both certain high- and low-skilled health-care workers. Immigrants accounted for 28 percent of the 958,000 physicians and surgeons practicing in the United States, and 38 percent of the 492,000 home health aides (see Table 1).
Table 1. All Civilian Employed Workers (ages 16 and older) and Health-Care Workers, by Occupational Group and Nativity, 2018
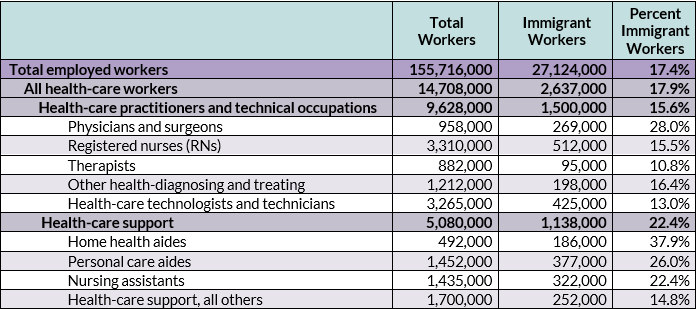
Note: The estimates of health-care workers here refer to their numbers by occupation, regardless of their industry of employment (many occupations can span several industries).
Source: Migration Policy Institute (MPI) tabulation of data from the U.S. Census Bureau 2018 American Community Survey (ACS).
The immigrant share of the health-care workforce was roughly twice the national level in three states: New York (37 percent), California (35 percent), and New Jersey (34 percent). Other states with high shares were Florida (30 percent), Maryland (28 percent), and Nevada (26 percent).
In a number of states, immigrants made up much higher shares of physicians and surgeons than of all health-care workers or all workers in general. In Michigan, for example, while immigrants accounted for just 8 percent of all workers and 9 percent of health-care workers, their share was three times as high (28 percent) among physicians and surgeons. Other states that have a relatively low share of immigrant workers overall while relying heavily on foreign-born physicians include New Jersey (39 percent), Nevada (38 percent), Florida and New York (36 percent each), and Massachusetts (34 percent).
Several states also had high shares of registered nurses who are immigrants: Nevada (36 percent), California (35 percent), Maryland (30 percent), and New York (29 percent).
In several states, immigrants accounted for large shares of low-skilled health-care workers, such as home health aides. New York had the highest share, with 75 percent, followed by New Jersey (55 percent), Florida (52 percent), Maryland (47 percent), and Massachusetts (45 percent).
More than 310,000 (or 12 percent) of immigrants employed in health-care occupations were humanitarian migrants, such as resettled refugees, asylees, special immigrant visa holders, and Cuban and Haitian entrants. These migrants were slightly less likely to work as physicians and RNs than other immigrant workers and slightly more likely to be in health-care support occupations (see Table 2).
Table 2. All Immigrant and Refugee Health-Care Workers by Occupational Group, 2018
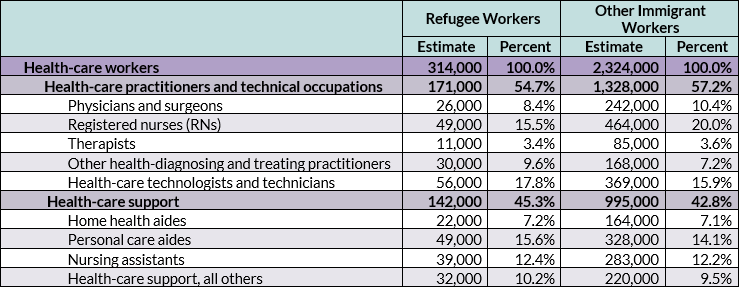
Note: The estimates of health-care workers here refer to their numbers by occupation, regardless of their industry of employment (many occupations can span several industries).
Source: MPI tabulation of data from 2018 ACS.
Regardless of nativity status, women were more likely to be employed as RNs and in health-care support occupations and less likely to be physicians and surgeons than men (see Table 3). Both immigrant men and women employed in health-care occupations in 2018 were more likely than their U.S.-born counterparts to work as physicians and surgeons: 25 percent and 5 percent of foreign-born men and women employed in health care, respectively, worked in these professions, compared to 17 percent and 3 percent of native-born men and women.
Foreign-born health-care workers overall were also more likely than their native-born peers to work as nursing assistants, personal care aides, and home health aides: For the foreign born, 38 percent of women and 19 percent of men worked in these occupations, compared to 22 percent and 14 percent of U.S.-born women and men, respectively.
Table 3. Occupational Distribution of Civilian Employed Health-Care Workers (ages 16 and older), by Nativity and Sex, 2018
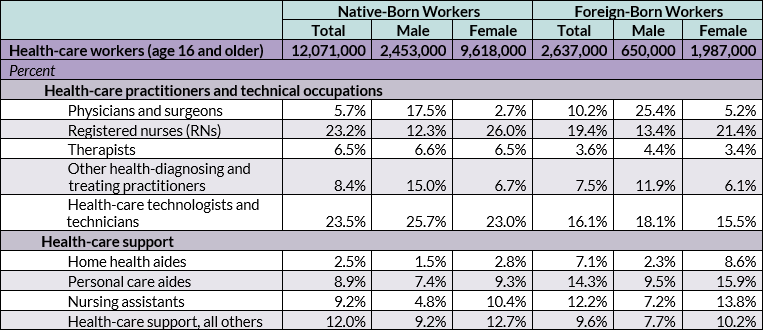
Note: The estimates of health-care workers here refer to their numbers by occupation, regardless of their industry of employment (many occupations can span several industries).
Source: MPI tabulation of data from the U.S. Census Bureau 2018 ACS.
Regardless of nativity, most health-care occupations rely on female workers. Women accounted for 75 percent of the 2.6 million foreign-born health-care workers in 2018. Among the native born, this share was even higher: 80 percent. Women represented the lion’s share of both foreign- and native-born registered nurses (83 percent and 89 percent, respectively). Similarly, both foreign- and native-born women accounted for approximately 88-92 percent of low-paid home health aides. In contrast, 38 percent of foreign- and U.S.-born physicians and surgeons were women.
Asia was the leading region of birth of immigrant health-care workers in 2018, with 40 percent, followed by the Caribbean (16 percent); Mexico and Central America (14 percent); Africa (12 percent); Europe, Northern America, and Oceania (12 percent collectively); and South America (6 percent).
Asian-born health-care workers and those from Europe, Northern America, and Oceania were more likely than their counterparts from other regions to work as physicians and surgeons and, along with those born in Africa, as registered nurses (see Figure 1). In contrast, 66 percent of immigrant health-care workers from Mexico and Central America, 60 percent from the Caribbean, 48 percent from Africa, and 47 percent from South America were employed in health-care support occupations.
Figure 1. Immigrant Civilian Employed Health-Care Workers (ages 16 and older), by Region of Birth and Occupational Group, 2018
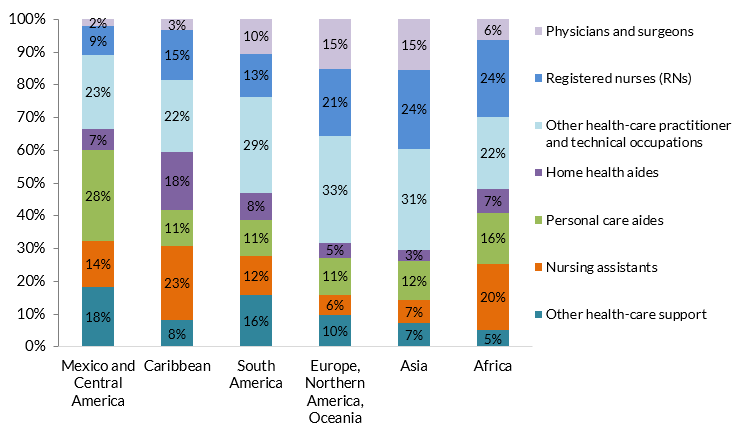
Note: The estimates of health-care workers here refer to their numbers by occupation, regardless of their industry of employment (many occupations can span several industries).
Source: MPI tabulation of data from the U.S. Census Bureau 2018 ACS.
Immigrants from the Philippines accounted for 28 percent of the 512,000 immigrants working as registered nurses, followed by those from India (6 percent), Nigeria (5 percent), and Mexico and Jamaica (4 percent each). Among the 269,000 immigrant physicians and surgeons, Indians were the top group with 22 percent, followed by those from China/Hong Kong (6 percent), Pakistan and Canada (5 percent each), and the Philippines (4 percent). Among 186,000 immigrant home health aides, the top countries of origin were the Dominican Republic (19 percent), Mexico (10 percent), Jamaica and China/Hong Kong (8 percent), and Haiti (6 percent). Mexico (21 percent), the Philippines (12 percent), and China/Hong Kong (6 percent) were the top three countries of birth of the 377,000 immigrants who worked as personal care aides.
Education, Naturalization, and English Language Proficiency
Foreign-born workers ages 25 and older in health-care occupations were somewhat more likely than their native-born counterparts to have obtained a bachelor’s degree or higher—49 percent, compared to 45 percent. This nativity gap in degree attainment was widest for health-care workers employed as registered nurses, health-care technologists and technicians, and "other" health-care support occupations (see Table 4).
Table 4. Educational Attainment for Overall Civilian Employed Population (ages 25 and older) and Health-Care Subset, by Occupational Group and Nativity, 2018
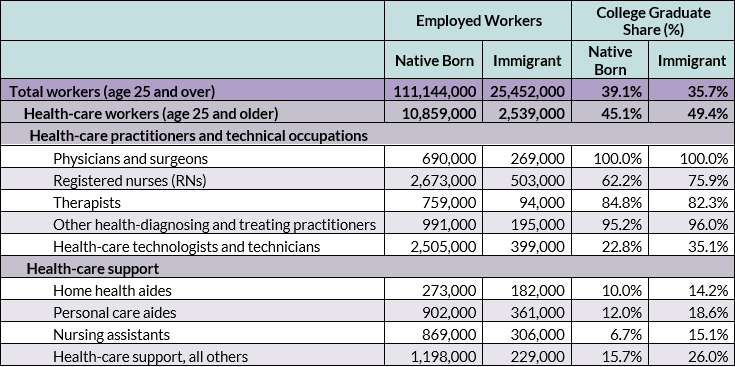
Note: The estimates of health-care workers here refer to their numbers by occupation, regardless of their industry of employment (many occupations can span several industries).
Source: MPI tabulation of data from the U.S. Census Bureau 2018 ACS.
The lion’s share of immigrant health-care workers were naturalized U.S. citizens: About 69 percent were naturalized U.S. citizens, compared to 51 percent of all immigrants in the U.S. workforce. The naturalization share varied by occupation, ranging from about 80 percent for RNs and other health-diagnosing and treating practitioners, 76 percent for physicians and surgeons, and 51 percent for home health aides (see Table 5).
Approximately 71 percent of foreign-born health-care workers reported speaking English proficiently, meaning exclusively or "very well." That English proficiency rate is markedly higher than for all civilian employed foreign-born workers overall, at about 56 percent (see Table 5). Most immigrants in the health-care practitioners and technical occupations reported high degrees of English proficiency. Less than half of home health aides and personal care aides were fully English proficient.
Table 5. Naturalization Share and English Proficiency of Immigrant Health-Care Workers (ages 16 and older), by Occupational Group, 2018
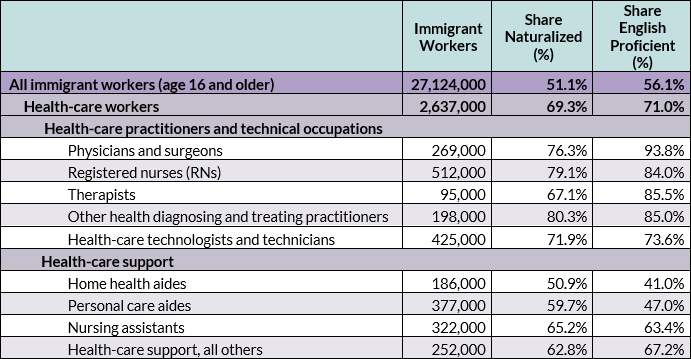
Notes: The term “English proficient” refers to workers who reported speaking English exclusively or "very well." The estimates of health-care workers here refer to their numbers by occupation, regardless of their industry of employment (many occupations can span several industries).
Source: MPI tabulation of data from the U.S. Census Bureau 2018 ACS.
Foreign-born health-care workers are admitted to the United States under a variety of temporary and permanent visa categories. Temporary visa categories include H-1B (specialty occupations), TN (Mexican and Canadian professionals under the North American Free Trade Agreement [NAFTA]), J-1 (exchange visitors), O-1 (persons with "extraordinary ability or achievement"), and E-3 (specialty occupation workers from Australia). As is the case with other immigrants, those in the health-care sector can be admitted through permanent immigration channels (i.e., getting a green card) based on family or employment connections, or through humanitarian protection routes.
It is hard to assess how many foreign health professionals arrive annually, whether via temporary or permanent visa channels, because for the most part visa data are not broken down by occupation. Since most occupations in health care require a professional license, relatively few foreigners meet the requirement unless they obtain a U.S. degree and complete the necessary postgraduate training first. Some doctors with foreign degrees are able to apply for a J-1 visa to complete a medical residency in the United States.
Despite the key role immigrants play in providing health-care services, the U.S. immigration system has not typically prioritized attracting foreign-born health-care professionals. Just 5 percent (or 4,771) of the 93,615 H-1B petitions approved for initial employment in fiscal year (FY) 2018 went to workers in occupations in health care and medicine, according to Department of Homeland Security (DHS) data. Fifty-one percent of annual H-1B petitions in FY 2018 went to workers in computer-related occupations.
Most workers employed in health-care occupations had health insurance in 2018, regardless of their occupation or nativity. A far greater share of immigrant workers in non-health-care occupations lacked coverage, compared to health-care workers: 22 percent versus 9 percent, respectively.
While the coverage rate was close to universal for physicians and surgeons and RNs regardless of nativity, about 13 percent of immigrant and 11 percent of U.S.-born health-care support workers lacked health insurance.
Sources
Batalova, Jeanne and Michael Fix. 2020. As U.S. Health-Care System Buckles under Pandemic, Immigrant & Refugee Professionals Could Represent a Critical Resource. Migration Policy Institute commentary, April 2020. Available online.
Fadel, Leila, Will Stone, Meg Anderson, and Robert Benincasa. 2020. As Hospitals Lose Revenue, More than a Million Health Care Workers Lose Jobs. NPR, May 8, 2020. Available online.
U.S. Census Bureau. 2018 American Community Survey. Accessed from Steven Ruggles, Sarah Flood, Ronald Goeken, Josiah Grover, Erin Meyer, Jose Pacas and Matthew Sobek. IPUMS USA: Version 10.0 [dataset]. Minneapolis, MN: IPUMS, 2020. Available online.
U.S. Citizenship and Immigration Services (USCIS). 2011. Temporary (Nonimmigrant) Workers. Updated September 7, 2011. Available online.
---. 2019. Characteristics of H-1B Specialty Occupation Workers. Washington, DC: USCIS. Available online.
U.S. Department of Labor Bureau of Labor Statistics. 2019. Employment Projections: 2018-2028 Summary. News release, September 4, 2019. Available online.